
June 16, 2026
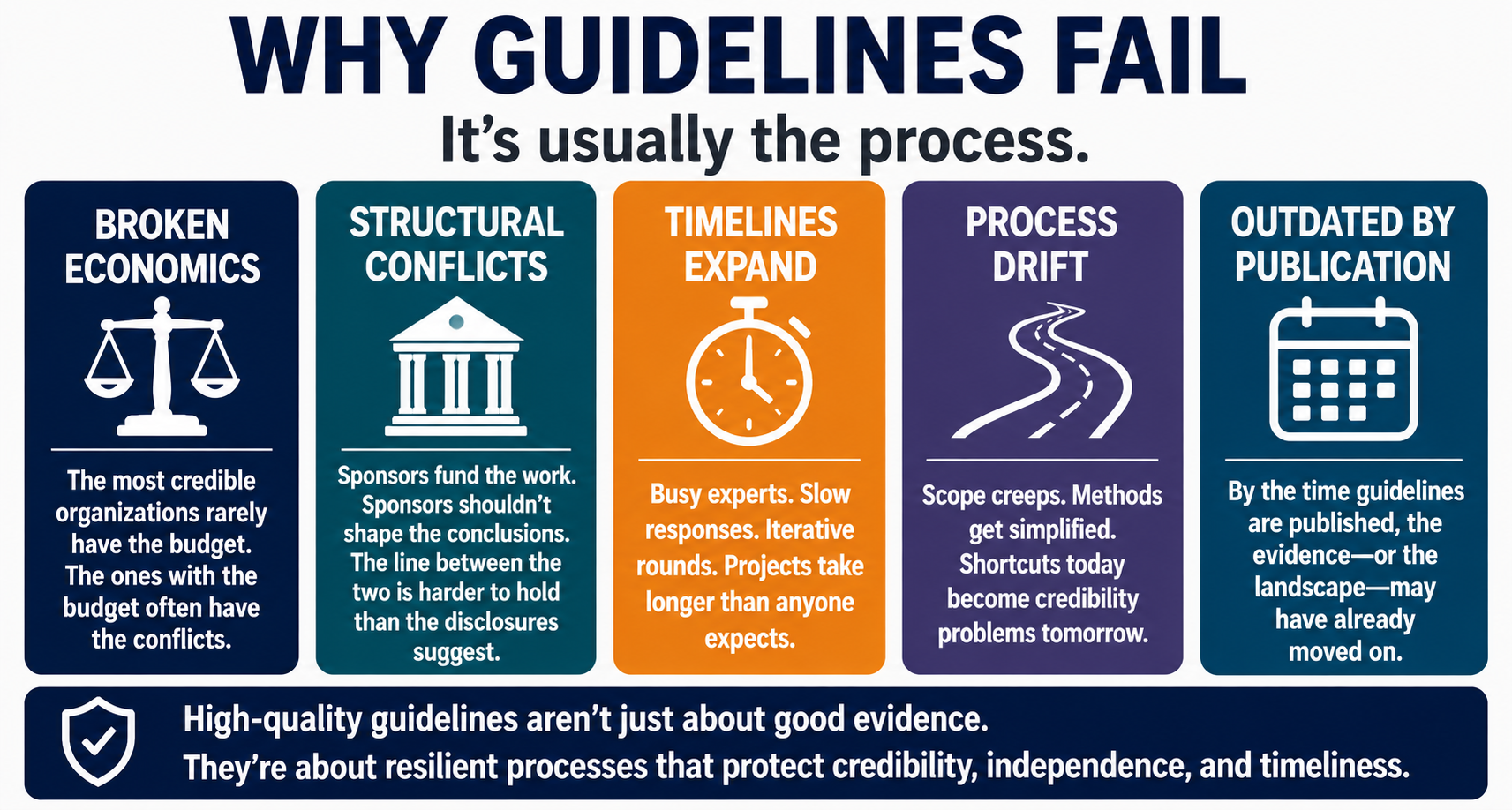
Many guideline failures are not failures of evidence alone, they are failures of process. Economic constraints, logistical complexity, and political realities exert a profound influence on guideline development, yet these forces are rarely discussed in the methodology literature despite being obvious to anyone who has lived through a guideline development process.
The previous posts in this series covered the frameworks, the tools, and the methods. This final post covers what the frameworks cannot protect you from: the systemic pressures that turn a six-month project into an eighteen-month one, that compromise independence without anyone intending to, and that explain why so many published guidelines score poorly on the very quality standards the field has spent decades developing.
These are not individual mistakes. They are predictable consequences of how guideline development is funded, staffed, and managed. Understanding them is the first step toward designing processes that resist them.
There is a fundamental mismatch between the organisations that most need clinical guidelines and the organisations that can afford to develop them properly.
The most rigorous guidelines require systematic literature reviews, formal evidence appraisal, structured consensus processes, multiple rounds of voting, professional medical writing, and months of iterative revision. That work is expensive. It requires specialised expertise: methodologists, medical writers, project managers, and sustained time from busy clinicians who serve as panellists.
Non-profit physician associations, academic consortia, and disease-specific foundations are often the most appropriate bodies to lead guideline development. They have the clinical credibility, the disease-area expertise, and the independence that lend a guideline authority. What they frequently lack is the budget to do the work at the level of rigour the field demands. In practice, many medical communications agencies, the firms best equipped to provide methodological and writing support, may deprioritise or decline consensus work because the economics do not support it. The result is a structural gap: the organisations with the most credibility have the fewest resources, and the organisations with the most resources often carry conflicts of interest that complicate the product.
This dynamic has a direct and measurable impact on guideline quality. As the AGREE II data discussed in Part 4 of this series demonstrated, rigour of development is consistently the weakest domain in published guidelines. That is not because panels lack expertise. It is because rigorous methodology costs money that many guideline sponsors do not have.
Industry sponsorship can be an important source of support for guideline or consensus projects, and it is not inherently problematic. Drug and device manufacturers have legitimate interests in ensuring that their products are used appropriately, and they often provide the funding that makes guideline development feasible when non-profit budgets cannot.
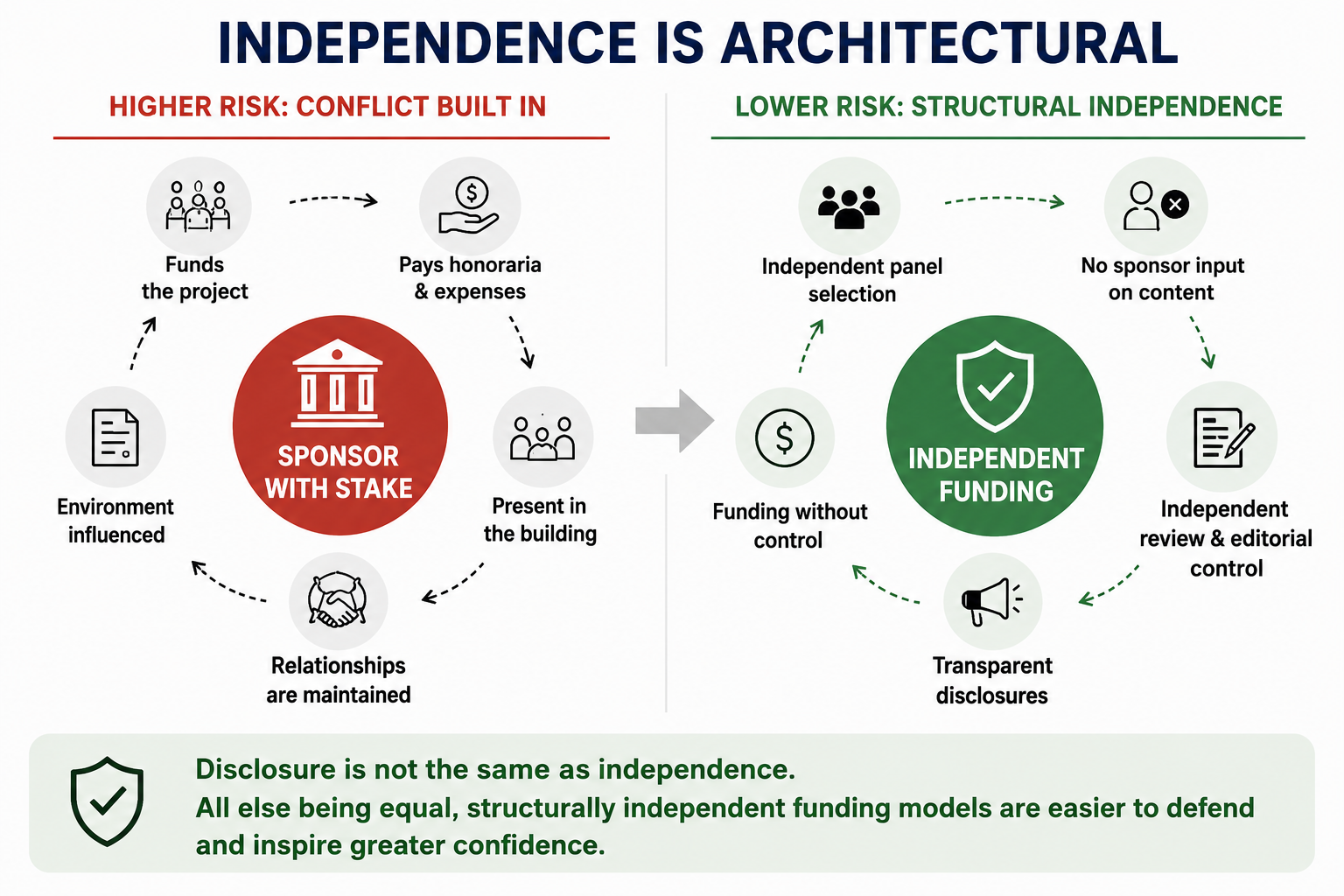
The problem is structural. When a single company sponsors a guideline that will make recommendations about how to use that company’s product, the conflict of interest is built into the architecture of the project, regardless of the intentions or behaviour of anyone involved.
The standard safeguards are well known: the sponsor should have no role in selecting the panel, no input into the recommendations, and no opportunity to review the manuscript before submission. In practice, the boundaries are more porous than the disclosures suggest. The sponsor funds the meeting. The sponsor pays the honoraria. The sponsor attends the dinner. The sponsor is in the room, not at the table where the voting happens, but in the building where the relationships are maintained. Even when the sponsor says nothing and does nothing to influence the recommendations, their presence can shape the environment in which the recommendations are made.
This is not an accusation of misconduct. It is an observation about incentive structures. The IOM standards require that the majority of the guideline panel be free of relevant conflicts and that the chair be unconflicted.1 These requirements exist because the field recognises that disclosure alone does not constitute management, and that even well-intentioned people are influenced by the context in which they work.
The most credible guidelines are often those that can demonstrate genuine structural independence, not merely through disclosure and conflict management plans, but through funding arrangements that minimise the potential for conflicts to arise in the first place. This is difficult to achieve but it is also increasingly what journals, policymakers, and clinicians expect.
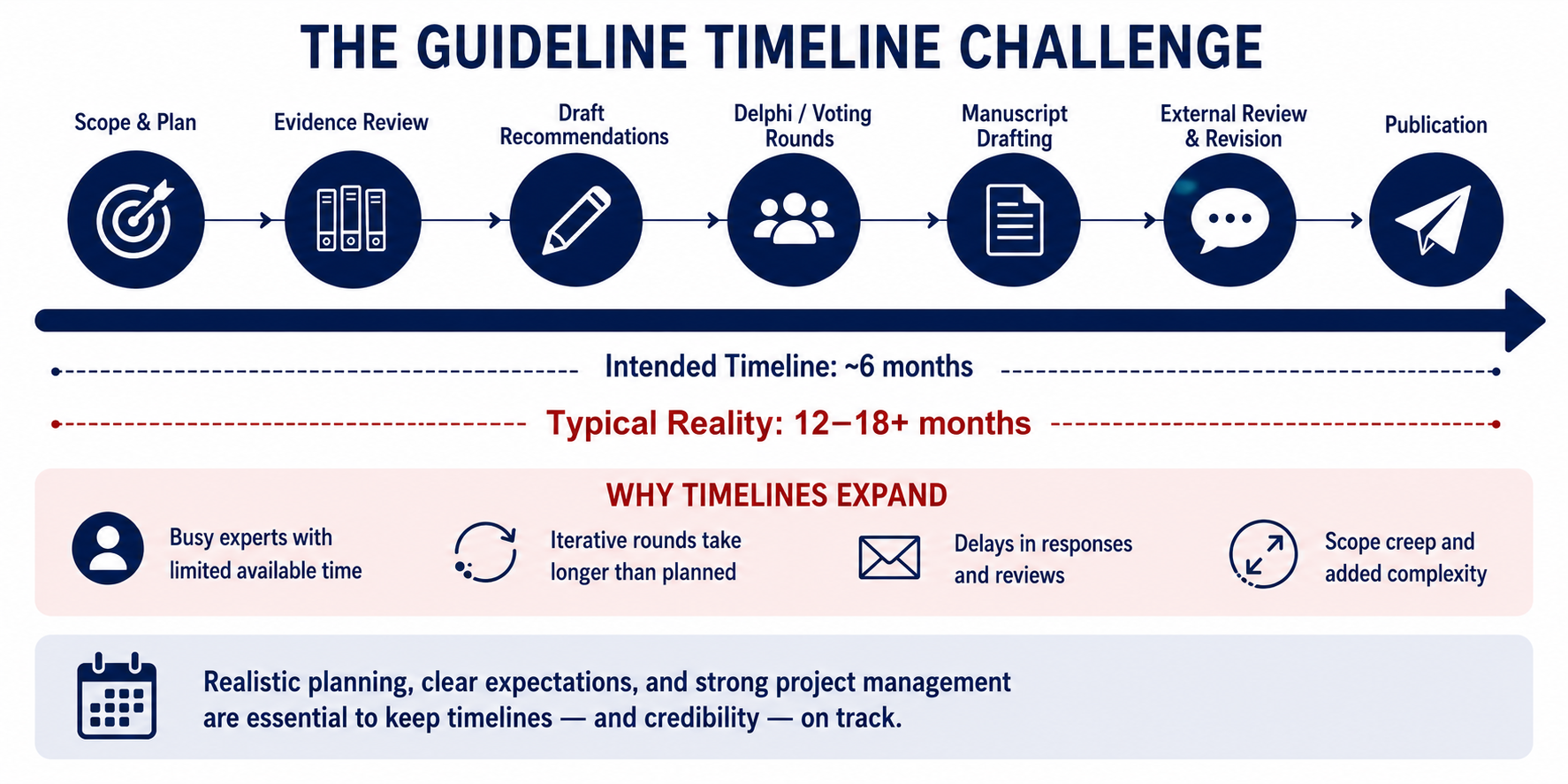
Ask anyone who has managed a guideline project what the single greatest source of delay is, and the answer is nearly universal: getting the panellists to respond.
The physicians and researchers who serve on guideline panels are precisely the people with the least available time. They are running clinical programmes, supervising trainees, managing their own research portfolios, and serving on multiple committees simultaneously. Guideline work, which is typically uncompensated or modestly compensated, carries no academic credit equivalent to a first-author publication, and involves iterative rounds of voting and review, competes for attention with everything else on their desks.
The consequences are predictable. Delphi voting rounds that should take two weeks take six. Manuscript reviews that should take ten days take a month. The second round of revisions generates an entirely new set of comments from a panellist who did not engage with the first round. A systematic literature review that was scoped for three months extends to nine as new studies are published during the delays and the panel requests that they be incorporated.
A project scoped for six months quietly becomes twelve. A project scoped for twelve becomes eighteen. The guideline that was supposed to be published before the society’s annual meeting misses the deadline and targets the following year’s meeting instead, by which time the evidence base may have shifted and the recommendations require updating before they are even published.
The structural remedy is not to find more responsive panellists, they do not exist in sufficient numbers. It is to design the process with realistic timelines, predefined response deadlines, a stated minimum response rate for each round to proceed, and a project plan that accounts for the fact that the people whose input matters most are the hardest to pin down.2,3
The panel convenes to address five clinical questions. By the second meeting, someone suggests adding a sixth. By the time the Delphi survey is drafted, there are twelve. Each new question requires additional literature review, additional discussion, and additional recommendation statements. The manuscript grows from a focused consensus statement into a comprehensive guideline that no one originally scoped, budgeted, or scheduled.
Scope creep in guideline development is not a failure of planning, it is a natural consequence of putting disease experts in a room and asking them what matters. Everything matters. Every clinical scenario is important. Every recommendation that is omitted is a potential gap in care.
The structural protection is a locked scope document, agreed upon by the panel before any content development begins. The scope should specify the clinical questions the guideline will address, the questions it will not address, and the process for adding questions if the panel determines during development that the scope is insufficient. Adding questions should be a deliberate, costed decision not an incremental drift that no one notices until the timeline has doubled.1
Guidelines are living documents, or at least, they should be. The IOM standards require a stated plan for updating, and AGREE II evaluates whether one exists.1,4 Most published guidelines include a sentence to the effect of “this guideline will be reviewed within five years.”
The reality is that many guidelines are rarely or never updated, and those that are often take so long to develop that the evidence base has shifted by the time they are published. The updating paradox is straightforward: the same structural forces that made the original guideline difficult to produce limited budgets, overburdened panellists, slow feedback cycles, make updating it even harder. The original guideline at least had the momentum of novelty. An update must compete for the same resources without the same enthusiasm.
Rapid or living guideline models, in which recommendations are updated continuously as new evidence emerges, have been proposed as a solution, with formal frameworks now established to guide their development.5 These models work well when the evidence base is narrow and fast-moving, as it was during the COVID-19 pandemic, when organizations including the WHO published dynamically updated guidance in near real time. For most therapeutic areas, where evidence accumulates gradually and clinical questions are broader, the traditional model of periodic review remains more practical, but only if the updating plan is realistic and funded from the outset.
The final structural problem is the one that ties all the others together. When budgets are tight, timelines are compressed, and panellist engagement is inconsistent, the methods section is the first thing to suffer. It is written last, often by someone who was not involved in the actual development process, and frequently reverse-engineered to describe a more rigorous process than was followed.
This produces the inconsistencies that peer reviewers identify and that AGREE II appraisals consistently flag: GRADE ratings without evidence profiles, a “systematic review” supported by a thin reference list, consensus methodology described but never implemented as described, conflict of interest disclosure without management.
The structural remedy, as discussed in Part 4, is a prospective methods protocol developed before the guideline development process begins, not after it ends. But the deeper remedy is to recognise that the methods section is not administrative overhead. It is the product. A guideline’s recommendations are only as trustworthy as the process that produced them, and the methods section is the only place where that process is visible to the reader.
Every structural force described in this post is predictable. That means every one of them is addressable by designing better processes from the start.
An independent funding model protects against the architectural conflicts of industry sponsorship. A locked scope document protects against creep. Predefined response deadlines and minimum participation thresholds protect against timeline expansion. A prospective methods protocol protects against retrospective rationalisation. And a realistic budget that accounts for the actual cost of rigorous methodology, rather than the cost that a non-profit can afford or that an agency is willing to accept, protects against the quality erosion that undermines the final product.
The organisations that produce credible guidelines are not the ones with the most resources. They are the ones that design their processes to resist the forces that compromise quality and that commit to methodological transparency even when it would be easier, faster, and cheaper not to.
That commitment is what separates a guideline that changes practice from one that gathers dust. It is also, in the end, what the 2,500-year journey from Hippocrates to Delphi has been about: the slow, difficult, ongoing work of ensuring that when experts agree on how to treat patients, the agreement is one that physicians and patients can trust.
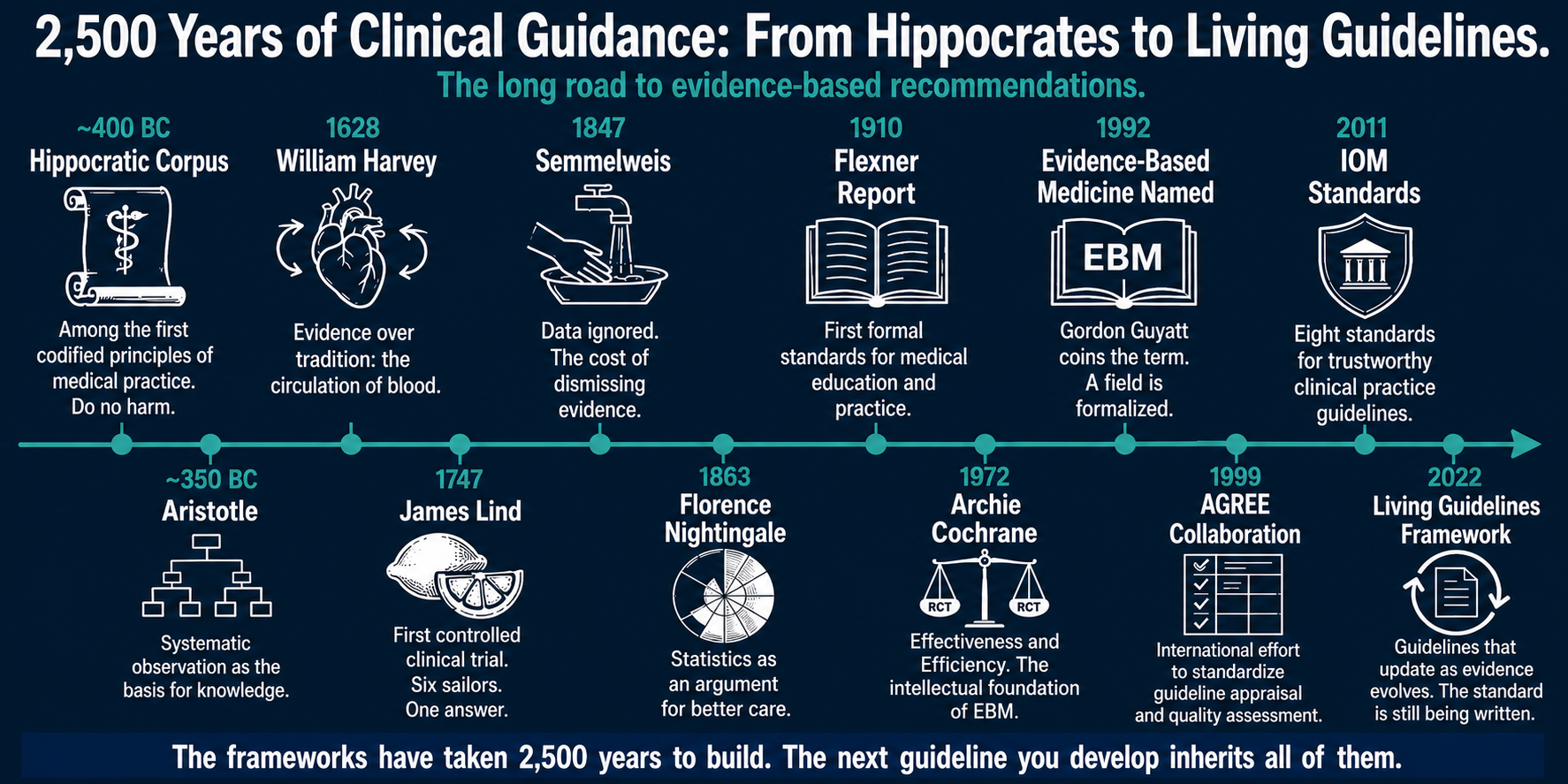
This concludes “From Hippocrates to Delphi,” a five-part series on the science and methodology of clinical guideline development.
References